CTN+ researchers seek to untangle how pain impacts patients’ day-to-day lives
Picture this: You wake up in the morning already sore. Pain shoots down your leg as soon as you try to get out of bed. You end up asking your partner to help. The shame is already creeping in, and worsens as you contemplate calling your boss to ask to work from home today; it’s that or brave a forty-minute commute on a busy bus.
This is the reality for eight million Canadians living with chronic pain. For those who are also living with HIV, the situation is even more complex.
Darren Lauscher is a patient partner with CTN 340, a study that is investigating those complexities and uncovering how people with HIV manage chronic pain in a society that so often ignores it.
Opening up
“What is chronic pain?” asked Lauscher. “Is it physical pain, or is it mental? Is it caused by the HIV, or did I do something to myself growing up?” The answers to those questions can vary hugely from individual to individual, and might have major implications on how best to handle that pain.
To find out, the research team, led by Dr. Franscisco Ibáñez-Carrasco at the University of Toronto, surveyed nearly 250 people living with HIV across Canada. They asked participants to rank statements about their pain’s impact on daily life, their concerns surrounding medication, and how stigma affects their wellbeing.
But statistical analysis can only take research so far — a topic as nuanced as pain needs to be understood in a human context, and that’s where Lauscher came in. He helped facilitate discussion groups among survey respondents. There were three groups: one for Spanish speakers/Latinos, one for gay and bisexual men, and one for women. Lauscher participated in the latter two groups as a narrator, ensuring that everyone could hear both the questions and responses, while fellow patient partner Kath Webster dug deeper.
“Being in a women’s only space is about first asking permission to be in the room,” reflected Lauscher. “But everyone proved to be very welcoming and forthcoming.”
The participants were asked to talk about their pain, not on an abstract scale, but how it impacted them day-to-day. Were they able to get out of bed in the morning? Go for a walk? Could they hold a 9–5 job? Did they feel judged by their friends and families for the things they couldn’t do?
“These were women who were research savvy, who have been researched a lot. And they said, ‘We’ve never had people really just respect us like this’,” said Lauscher. “They had never been in a position like this before, where the process was interactive, where we allowed them a space to have conversations around some really raw stuff about their pain.”
Early findings
The information collected from the survey and conversations are still being analysed and interpreted. But while the publication process is underway, Lauscher and fellow patient partners Kath Webster and Claudette Cardinal presented the study’s initial findings in a poster at the Patient Voices 2025 conference.
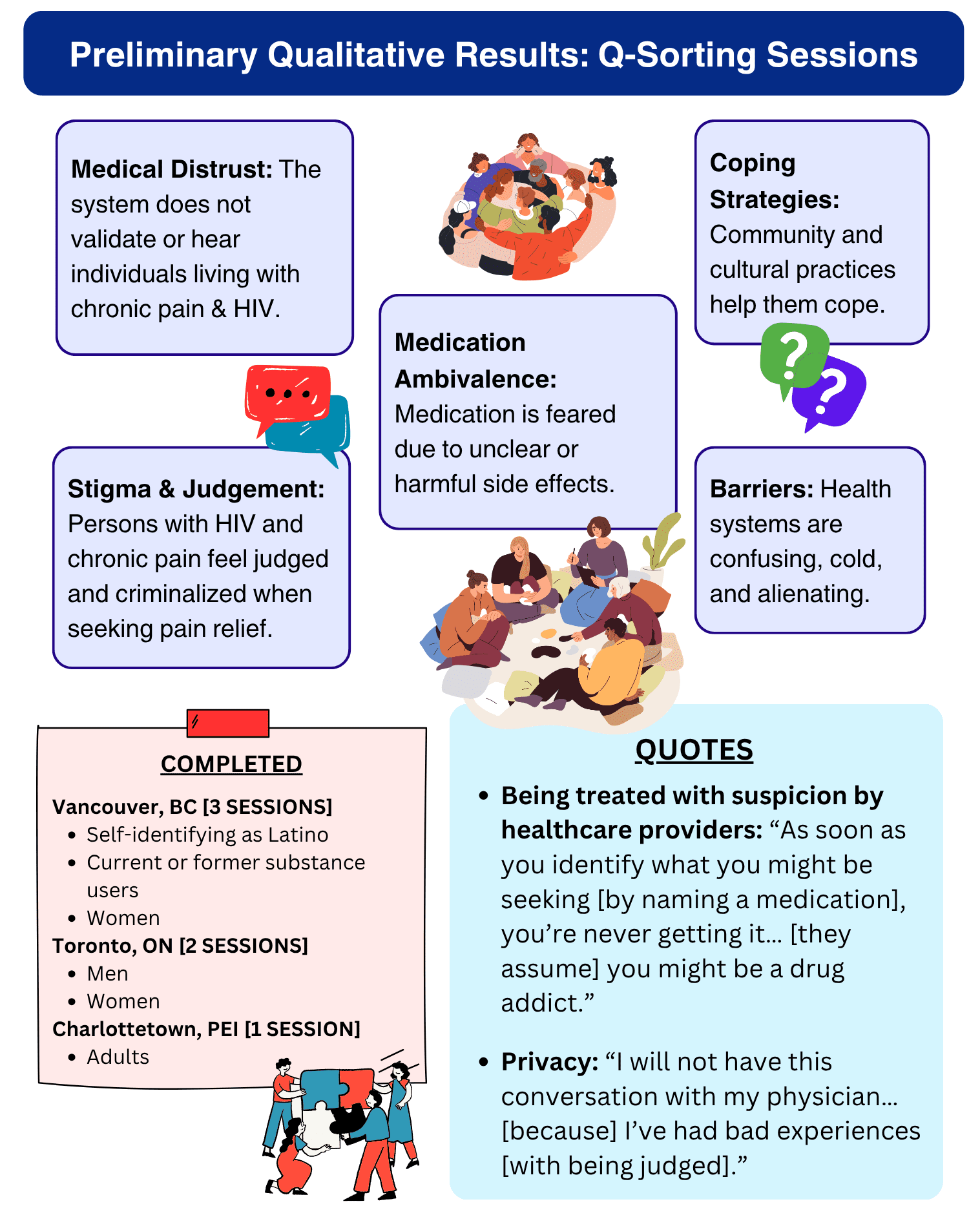
Initial analysis of the qualitative results has found participants’ attitudes coalesced around five central themes:
- Medical distrust
- Stigma and judgement
- Medication ambivalence
- Coping strategies
- Barriers to health care
Lauscher shared how these themes capture the profound, multi-faceted ways these topics impact participants’ daily lives.
To self-medicate or not?
Everyone living with chronic pain finds ways of managing it, but those strategies can differ from person to person. Lauscher explained, “What we heard in the discussion groups is that a lot of it is connected to social determinants of health — whether you have housing, food security, health care, or the ability to maintain your medication regimes without issue.”
Canada is now over a decade into the opioid crisis. Pain support prescriptions are often restricted by health care providers attempting to limit people’s chances of becoming addicted. That means making judgement calls about who’s allowed to access pain relief. In some cases, the complex history and connection between HIV and injection drug means that these medications are not accessible to everyone who might need them.
Lauscher believes an outright rejection is not the answer. “If someone is labeled a drug seeker, we need to be asking: what aren’t we doing right in our healthcare system that’s got them into that position?” said Lauscher. “Has our denial just become part of the pain process?”
When people cannot access pain support through official health care channels, they find ways to self-medicate. That might be in the form of alcohol, marijuana, or other drugs. While self-medication can be crucial for managing day-to-day, participants described how this can lead to a dangerous cycle: “You’re chasing that pain avoidance by self-medicating, and the self-medication only works for a certain amount of time before you become ‘resistant’. Then you have to up your doses and start chasing the next high to take you out of the pain,” he paraphrased.
Exercise as a double-edged sword
Participants also discussed some healthy strategies to help with their pain symptoms, but shared how it isn’t always so straightforward. Exercise is often touted as a method to help manage and mitigate chronic pain, and for good reason. “We do know physical exercise is good for us in moderation, and only becomes more so as we age, since it has implications for joint lubrication, heart issues, breathing, balance, and more,” said Lauscher. “But through it all, you’re still in pain.”

Exercise can be expensive; a gym membership can easily cost $30 to $200 per month. Furthermore, the benefits of exercise can quickly become a catch-22. “Are you able to actually do physical exercise or are you in a position now where that’s just too hard?” asked Lauscher. “Maybe your weight is too much, your knee joints hurt, your hip joints hurt.” The people who could benefit the most from exercise are the same ones barred from it.
Certain exercises are often promoted as being low-impact, and therefore easier for people living with chronic pain. But even those options fall short. “Somebody said to me, ‘Well, go swim’.” Lauscher laughed. “That works for some people, but if you don’t like water, or you sink like a rock, swimming is not enjoyable. In fact, it’s kind of scary.” Body image and the physical inaccessibility of pools also become issues. Lauscher said, “Sometimes people wonder, if I get in the pool and I get into trouble, who’s going to be there to help me?”
There’s another complicating element to exercise. While it provides many varied health benefits, when overdone, or done incorrectly, it can cause injury — and make the pain worse.
“It can be dangerous when someone exercises themselves to the point of exhaustion,” said Lauscher. “Or hurt themselves chasing ‘the Runner’s High’ or ‘the Gym Bunny’ high. Adrenaline becomes its own form of pain management.”
Knowledge is power
“At the end of the day, we really do need more information and understanding of how the body works and why HIV does what it does,” said Lauscher.
Are the higher rates of chronic pain found in people living with HIV a consequence of the virus itself? A side-effect of their treatments, such as the nerve pain (neuropathy) caused by ART? Or the inevitable consequences of aging that all people experience? Or is it an accumulation of all these factors?
Researchers are still trying to untangle the answers to those questions. The work being done by the CTN 340 team is part of that piece. They are currently analysing the results from the discussion to better understand the top priorities of people living with both HIV and chronic pain — and how to better adapt systems to support them.
“At the end of the day, a little pain is not a bad thing,” Lauscher said, smiling ruefully. “It makes you realise you’re alive.”
But that only goes so far. If there was one message Lauscher hoped health care providers would take away from the research, it is this: “Take it seriously when your patient is telling you they have pain. Take it seriously and investigate it. The health system is not designed to fix some of this stuff. Acknowledge that and come up with a care plan that recognises that reality.”
Want to learn more about the intersection of chronic pain and HIV? Hear Darren Lauscher and Kath Webster speak at an upcoming webinar on April 1st. If you’ll be in Winnipeg for April 22nd, join like-minded community members for a 2 hour interactive scavenger hunt with the event ‘Winnipeg Walks: HIV, Pain, Care & Community’.